


Our Services
| Clinic for Head & Neck Reconstruction | ||
|---|---|---|
Clinic for Head & Neck Reconstruction
Head and neck cancer has been increasing because it has come to an aging society with increased population of smoking and drinking. It is not easy to detect the head and neck cancer early enough to be cured because it has rare specific early symptoms. Head and neck cancer including brain tumor, salivary gland tumor, tongue cancer, paranasal sinus tumor, neck caner, and aerodigestive tract cancer may accompany the facial deformity following the resection of the cancer. In this case, serious functional deficit follows and empty space or dead space that has to be occupied with other soft tissue to restore the function. Furthermore, it can cause serious functional deficit after the cancer is resected completely. Plastic surgeon gives strong support for the reconstruction of the defect following the tumor resection otherwise it will be hard for the neurosurgeon or ENT surgeon to make sure the complete excision. That is to say, if the defect is small, reconstruction is possible using the adjacent tissue. On the contrary, if the large defect cannot be avoided, it is necessary to transfer the distant tissue. In addition, reconstruction of the head and neck should fulfill the need of functional restoration as much as possible. It takes some times to restore full function and rehabilitate following the surgery. Degree of functional recovery depends on the location and dimension of the defect. Nowadays, remarkable improvement of the microsurgical technique can make free transfer of the autogenous tissue possible and minimize the cosmetic and functional deficit as well as guarantee the complete wide excision. Free transfer of the tissue using the microsurgical technique is the operation that comprises elevation of the necessary tissue from the donor site such as arm, thigh, and abdomen with the vascular pedicle and microanastomosis to the recipient vessel and coverage over the defect site according to the site and defect size. Because the vascular diameter is approximately 1 to 2 mm, refined microsurgical technique is essential and it takes longer time. However, thorugh this kind of free flap surgery, the fittest type and shape of tissue can be designed for the defect site and transferred, therefore various versatile reconstructions are available and postoperative functional recovery including the food intake and pronunciation.
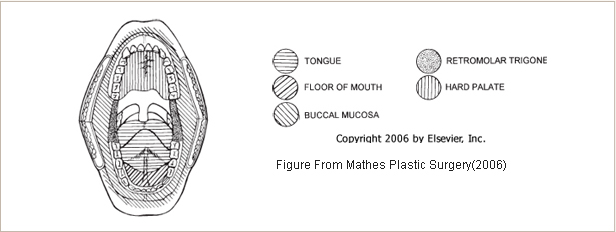
Defect resulting from the resection of the head and neck cancerDead space in the cranium, oral cavity, orbit is not obliterated spontaneously and can be the trigger factor of infection so that the tissue with adequate size should be used to fill the defect from the chest, back, and temporal area.
Facial nerve palsyFacial nerve palsy occurs frequently with the removal of the brain tumor or parotid gland tumor. If the injury occurs, neurorrhaphy or nerve graft can be tried. If the paralysis has persisted long, free transfer of the muscle can be another option to reanimate the facial expression..
Lagophthalmos
Facial expression Restoring the facial expression, also referred to the reanimation, is very hard and even if the optimal surgery is performed, fine expression is unable to be recovered. Apparent facial asymmetry in resting state especially on the lateral canthus and commisure of the lip can be partially corrected with traction and fixation of the involved area. For the full restoration of the facial animation, reconstruction of the nerve and muscle should be considered. If the time interval is not long after the facial nerve injury so that it does not cause atrophy of the facial muscle, nerve graft can be tried. If it has passed 1 to 2 years following the facial nerve injury so that there is overt facial muscle atrophy, free tissue transfer including the muscle, nerve with the vascular pedicle is necessary.
|
||

- Previous
- Craniosynostosis & Facial Asymmetry
- Next
- Polydactyly & Syndactyly

